Hendy and I had a comprehensive meeting today with our supervisors Jon Patrick, Alan Fekete and Peter Budd (a PhD student who developed G.H.I.M.S and Terminology Server).
Administration
Over the next 6 weeks, Jon Patrick will be away. Temporarily taking his place as thesis supervisor will be Alan Fekete (refer to previous posts). We plan to keep in touch with Jon through regular email and progress updates on the TRAC website. We have also set up weekly meetings with Alan Fekete every Thursday at 12 mid day.
Project as of today
So far, the system analysis phase of the project has been finalised. Only minor changes need to be made which will take no longer than a couple of days. However, we are still perfoming some validation and feedback tests with Angela at the RPA (she has been unavailable this week). With the first half of the project complete, Hendy and I will diverge in our investigations in the remainder of the second phase of the project.
Project Goals for the remainder of the thesis (Project Scope)
Generally, the aim of the project is to develop a working prototype that demonstrates (a proof of concept) a document centric workflow management systems in an ICU environment.
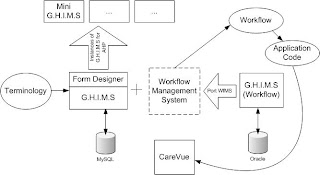
The diagram above depicts the current state of the technology. Essentially, there are two versions of G.H.I.M.S that need to be consolidated. The version of G.H.I.M.S that was developed by Peter Budd contains a form designer with version control using a MySQL database. The second version of G.H.I.M.S, developed by William Chau, contains a workflow management systems (WfMS), written in C#, but does not contain a versioned form designer. The backend operates on an Oracle database.
In order for the system to function, investigation needs to be done to port the WfMS into Perl for it to be compatable with G.H.I.M.S developed by Peter. Open source backend, such as MySQL will also need to be implemented. Using the system and workflow analysis completed in the first half of the thesis, we have to demonstrate the generic generation of an ICU information system. In order to reduce scope, this ICU system will be a component of the ideal system that is complex enough to demonstrate a proof of concept. It is essential that several principals, on which G.H.I.M.S is based upon, are demonstrated. These are (on the top of my head):
- Support for user workflow - adaptive workflow for the main users of an ICU information system; i.e., clinicians, nurses, allied healthcare professionals, administrators, researchers
- Use of terminology (SNOMED-CT)
- Customisation and Interoperability - data transfer between the ICU G.H.I.M.S and a mini (basic) G.H.I.M.S for allied healthcare professionals.
- Extendability - ability for users to effectively define their own systems (and workflow) with the use of the form designer.
- Medical Record storage and retreival.
My Tasks for the next week
For the following week, I plan set up the development environment on my laptop, install Peter's code and experiment with G.H.I.M.S. (I have scheduled a meeting with Peter Budd on Friday). My specific aims is to see what is required in order to make the system (bar the WfMS) to work with CareVue or to be able to mimic CareVue. This requires investigating the paper and electronic document environment surrounding the ICU's workflow and their use with CareVue and possibly, how adaptive their workflow will need to be. I plan to post an entry on adaptive workflows soon as this area is especially useful in the ICU environment.
Draft Treatise Hand In
I have finalised the draft treatised and given a copy to Alan Fekete and Jon Patrick for initial feedback. Over the next two days, I plan to work on the draft treatise extending the system analysis and workflow analysis chapters. I also have to clean up the literature review and continue to add to the literature base as I continue researching.










