Today Hendy and I had a meeting with Alan Fekete and Peter Budd to report our findings for the previous week and discuss how we could divide up the treatise into two meaningful segments.
The following segment describes the findings describing whether the G.H.I.M.S ICU system will rely or use CareVue.
Investigation into the use of CareVue in G.H.I.M.S ICU
The following segment describes the findings describing whether the G.H.I.M.S ICU system will rely or use CareVue.
CareVue Database Environment
- Data is recorded by CareVue and stored into two separate databases; real time database and an historical database. The difference in both databases is that the real time database records and displays live data for recent ICU patients whereas, the archival database stores data for all ICU patients.
- The historical database is called the Information Support Mart (ISM); a clinical data management information support mart that interfaces with CDA to create a set of approximately 30 tables from 300 tables.
- The real time database is called the Clinical Data Archive (CDA) contains over 300 tables
Extraction of Data from CareVue for the ICU G.H.I.M.S
- Currently, there is code written (from another project called the Ward Round System) to extract data from the historical database. As a result, we envisage that investigation into extracting data from CareVue and inputting it into an ICU G.H.I.M.S would be trival.
- While extracting data from CareVue would be achievable, inputting the data into the database is live or archival database is problematic because:
- We will be manipulating
- There is a resource constraint on the access of the database.
- Furthermore, it is envisaged that the complete ICU G.H.I.M.S would serve as a replacement to the hospitals current information system setup. Instead, de-identified CareVue data could be used as a base for data requirements analysis (as per system analysis completed) and as sample data to enter into a prototyped ICU G.H.I.M.S.
Workflow in the ICU
- CareVue currently does not support a workflow management system.
- There are really no standardised forms that CareVue uses during throughout the workflow in the ICU. There are certain stages and activities (e.g. automated recording of vital signs, recording of nurse discharge summaries) where there are computerised forms which are later printed out. A significant portion of clinician notes a rerecorded in free text, however some entries follow standard template (such as the Ward Round Templates).
- Some paper forms are used during certain ICU workflows. For example, during the discharge process, medication data in CareVue is transferred by the nurse and doctors to standardised forms which are used hospital wide.
Conclusions
The Workflow Management System

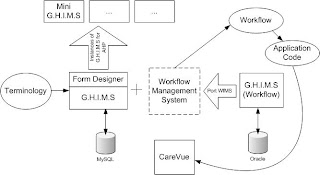
The workflow management system (shown in diagram above and in previous post) can be divided up into two independent sections - a workflow builder and a workflow manager. The workflow builder will allow users to create abstract workflow representations which then can be instantiated by the workflow manager. The workflow manager will then require to route the workflows to the appropriate users at the appropriate time. The workflow builder and workflow manager becomes the foundation for the proposed workflow management system.
The need for a workflow managment system, workflow builder and workflow manager requires some form of common ground for communication between each segments. Therefore a workflow definition language written in XML would need to be devised. This would be served as a set of rules used to describe workflows in XML much like the FDL (Forms Definition Language).
Task for the following week
For the following week, I plan to do the following:
For the following week, I plan to do the following:
- Hendy and I are to work on the workflow definition language.
- Investigate requirements and scope for the workflow builder and workflow manager.

{kind=link}